How a Clinical Operations AI Agent Works: The 5 Things It Does That Your Team Doesn’t Have Time For
The question we get most often in the first conversation with a healthcare operations leader is not ‘can AI do this?’ It is ‘what exactly does it do, and what does it replace?’
That is the right question. And the answer is specific.
A clinical operations AI agent replaces the manual work that happens before the judgment. The reconciling, the assembling, the waiting-for-the-report work that consumes hours every week and still produces outputs that are stale by the time anyone reads them.
USM Business Systems builds clinical operations AI agents for mid-market health systems, specialty pharmacy groups, and pharma and CRO organizations. Here is what those agents actually do.
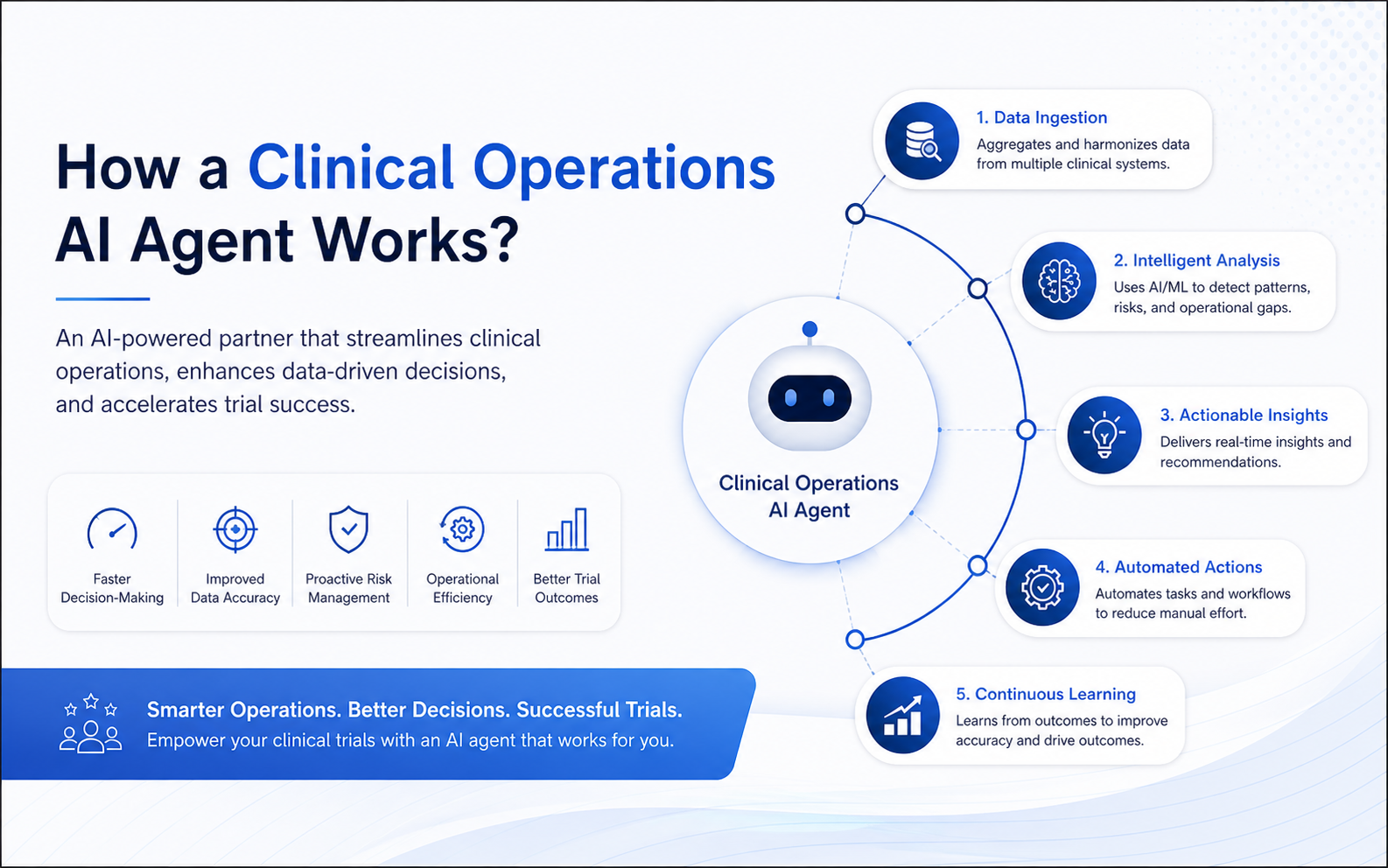
1. Continuous Data Reconciliation
Most clinical operations teams reconcile data manually. Prior auth statuses from payer portals. Prescription intake status from the pharmacy management system. Patient eligibility from the clearinghouse. Claim status from the EHR billing module. All of it arriving at different cadences, in different formats, from different systems.
The agent handles all of that continuously. Authorization statuses update when payer decisions come through. Prescription intake positions update as processing completes. Eligibility verification updates as clearinghouse responses arrive. The team opens the dashboard and the picture is current.
- Time recovered: 4–10 hours per coordinator per week
- Decision quality improvement: leadership briefs off data that is hours old, not days old
2. Automated Exception Surfacing
The most expensive clinical operations problems are the ones nobody noticed until they became denials or delays. A prior auth that has been sitting in a payer queue for eight days. A specialty drug with a procurement constraint that is not visible in the formulary system. A patient eligibility issue that will generate a claim denial 30 days from now.
The agent monitors the operation continuously and surfaces exceptions automatically. It does not wait for the weekly review. It flags the situation when the threshold is crossed.
- Near-miss visibility window extends from hours before a denial to days before
- The team shifts from reactive denial management to proactive issue resolution
3. Root Cause Analysis on Demand
When a clinical operations problem occurs, the investigation typically takes longer than the resolution. Where did the breakdown start? Which payer? Which authorization type? Which upstream data signal was the leading indicator?
The agent traces disruptions backward through the data and presents the cause with supporting evidence. The operations director does not spend Monday morning running the investigation. They receive the analysis and move to the response.
- Mean time to root cause: reduced from days to hours
- For specialty pharmacy operators where a single denied specialty drug claim runs $10K–$80K, this is direct margin protection
4. Plain-Language Scenario Modeling
Healthcare operations decisions under uncertainty require modeling. What happens to authorization approval rates if Payer A changes their criteria next quarter? What does adding a second specialty drug to the formulary do to procurement timelines and patient wait times? What is the revenue exposure if denial rates on this service line hold at the current pace through Q3?
Historically, running those scenarios required an analyst, a spreadsheet, and time that is usually not available before the decision needs to be made.
The agent accepts plain-language questions and returns modeled answers. The revenue cycle director or pharmacy director asks the question and gets the output in minutes. The decision is made with the modeling, not in spite of the absence of it.
5. Automated Reporting and Narrative Generation
Weekly ops reviews, payer scorecards, and executive summaries do not disappear when a clinical operations agent is deployed. What changes is who builds them.
The agent generates those reports automatically, from the live data it is already reconciling. The narrative is written. The tables are populated. The anomalies are flagged.
The clinical operations team does not spend Thursday building Friday’s report. Reporting becomes a byproduct of operations, not a project with a deadline.
- 4–8 senior team hours recovered per week on report assembly
- Version control and manual error risk eliminated from compliance-sensitive reporting
What the First Deployment Looks Like
The teams that get the most out of clinical operations AI identify one specific problem and run a contained build on it first.
USM scopes every healthcare AI engagement in two weeks. We identify the one or two problems with the clearest ROI and the fastest measurement cycle. We build to that scope. We measure from week one.
Most first deployments are live within 8–12 weeks. The team starts using the output before the quarter is out.
Request a 30-minute Clinical Operations AI walkthrough at usmsystems.com. See the live system, not the slide deck.